

Head and Neck Robotic Surgery
Head and Neck Robotic Surgery
Minimally invasive surgical techniques have been recently developed in an attempt to avoid lengthy surgical procedures, extended post-operative recovery and to ensure better esthetic results, decreased iatrogenic trauma and well-tolerated procedures. Endoscopic surgery was advanced, increasing surgeons’ capabilities in serving this purpose. Although it was a big step towards minimally invasive surgical philosophy, it had some challenges and limitations. Robotic-assisted surgery was introduced in 1985 as a part of this effort, aiming to overcome some of the limitations of the conventional endoscopic surgery. In its first application, it was used for neurosurgical biopsies. Since then, a large group of medical specialties such as general surgery, urology, cardiothoracic surgery, gynecology, orthopedic surgery, and neurosurgery, have been using the Robot for an increasing number of surgical procedures. The application of robotic-assisted surgery in the Head and Neck area was initiated very recently.
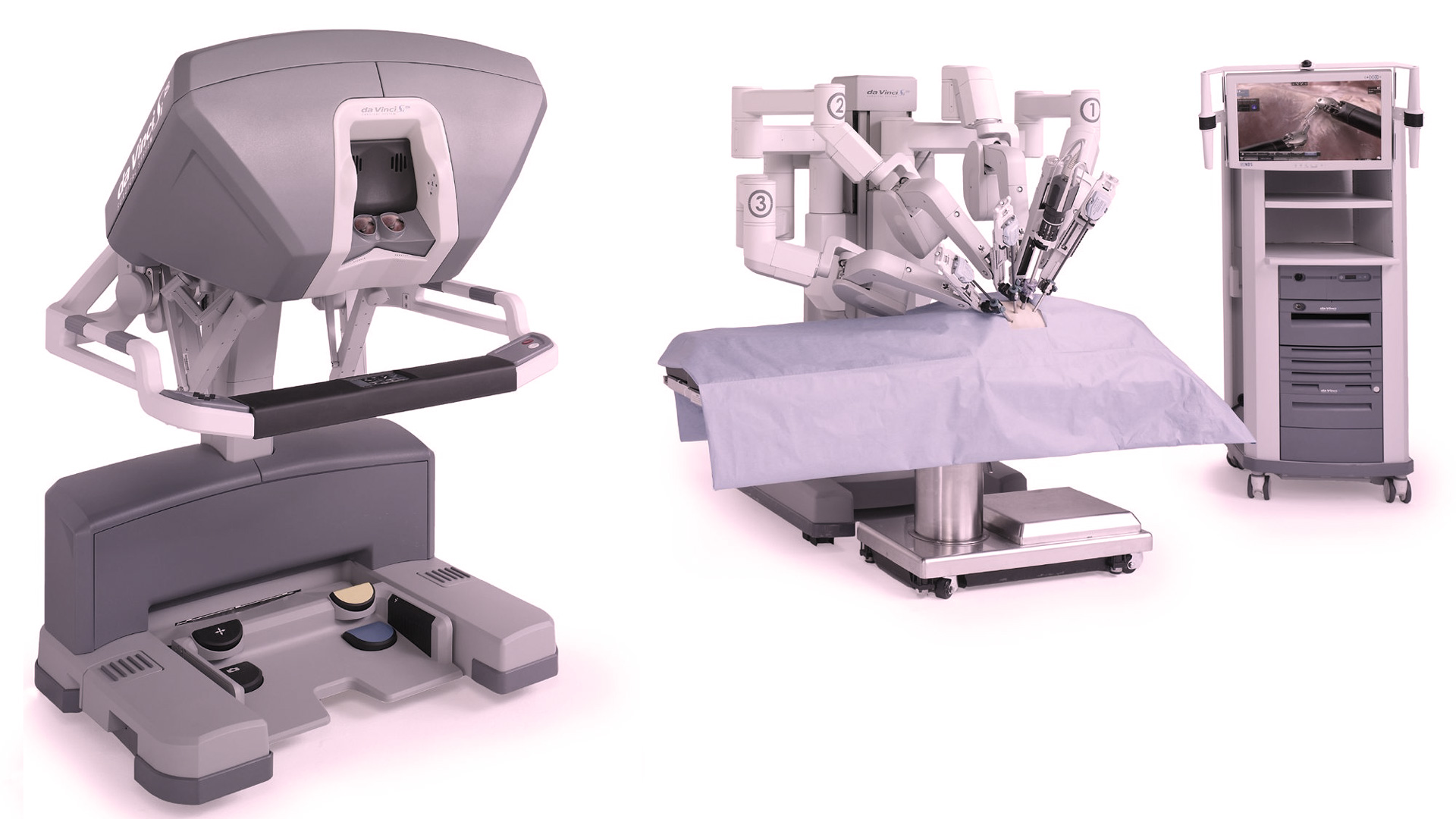
The Surgical Robotic system is a comprehensive master-slave arrangement, with the robotic surgical cart containing multiple manipulation arms that are operated remotely from a console. The robot is composed of three main parts: the surgical cart, the vision cart, and the surgeon’s console.
The advantages of robotic-assisted surgery are:
1. Enchased visualization of the surgical field
2. Elimination of physiologic tremor
3. Multi-articulated instruments
4. Reduction of the surgeon’s fatigue
5. Proper eye-hand coordination
6. Possibility for Telesurgery
The main disadvantages are: the cost of the robotic system, the size and weight of the equipment, the absence of haptic and tactile sensation and the fact that its benefits compared to the traditional techniques are still a subject of research.
Transoral Robotic Surgery (TORS) is defined as a procedure performed via the oral cavity, during which three arms of the robot are used, and bimanual handling of the tissues is possible. The first transoral robotic surgery was performed in 2005, and in 2009 the Da Vinci Robotic system became FDA approved for transoral surgical procedures. This exciting technology is new in the field of intraoral surgery. It is gaining popularity during the last 6-8 years, as it provides several advantages compared to the traditional surgical techniques. One of the undoubted advantages is the access to certain areas, like the base of the tongue or parts of the pharyngeal walls, where conventional instrumentation is difficult to reach. The enhancement of the visual field by tenfold magnification, as well as the three-dimensional view, offers great assistance to the surgeon. Distinguishing the types of tissues during oncological dissection and avoidance of damaging important structures such as nerves and vessels is greatly facilitated. Robotic surgery is also associated with decreased operative times and hospitalization, less morbidity (infection, pain), excellent functional outcomes and faster return to normal activities.
TORS may be used for benign and malignant lesions of the base of the tongue, the palate, the palatine tonsils, the parapharyngeal space, the posterior and lateral pharyngeal wall, the floor of the mouth, the retromolar trigone, the larynx, and the hypopharynx. Patients with sleep apnea due to excessive lymphoid tissue or true muscle enlargement at the base of the tongue may also benefit from a robotic-assisted debulking. Vascular lesions extending in areas where direct visualization is problematic may also be meticulously dissected with the use of the robotic system. As experience is now accumulating from many different centers throughout the world, the application of robotic assistance in Head and Neck Surgery will continue to expand.
Not every patient is a candidate for Robotic transoral procedures; reduced mouth opening, the configuration of the dental arches, incomplete lesion visualization, mandibular involvement, tumors involving >50% of the base of the tongue or the posterior pharyngeal wall, the internal carotid artery, or the prevertebral fascia are contraindications for TORS.
Performing a transoral robotic surgery requires first of all training and experience of the surgeon and the assistant surgeon. The anesthesiology team has also to be trained as there are some alterations of the anesthesia organization and set up. Additionally, the scrub nurse and the circulating nurse must also be familiarized with the procedures. The rest of the operating room personnel must also be experienced. Finally, the surgical team has to have access to all the appropriate instrumentation from the market and the overall support of the company.
Dr. Tombris was awarded the diploma of Robotic surgery (accredited by the European Accreditation Council for Continuing Medical Education) from the University of Lorraine, Nancy, France. He is one of the few Maxillofacial Surgeons with similar training.
We will be happy to discuss the option of a transoral robotic procedure for particular cases with our patients if the criteria of including this exciting new technology to our treatment planning are met.